Perhaps I went into this for all of the wrong reason(s)?
Maybe not the wrong reasons, but, perhaps the expectations were unrealistic? Maybe there was too much of me in this endeavor for others? Maybe it's the other way around?
These are the questions I ask myself as I muck through the maze of my daily life as a veterinarian in general practice.
 |
| One of the many delightful faces of my vet life day |
Yesterday I spent a long time, (to be honest 20-30 minutes), with a sobbing client as she dropped off her dog, Brunswick, for a forelimb amputation. She was, (as every single other amputation pet parent has ever been), reluctant to consent to this surgery. Of all the procedures that we do, and, for all of the many indications this procedure is recommend for, there is no other life-saving, pain alleviating surgery that is met with such pet parent reluctance and resistance. In my clinic over the last 15 years that I have been practicing, I would say that only about 1/4 of the pets who need this procedure, and, I believe would benefit immensely from, actually get it. Most pet parents will sacrifice the pet to spare the removal of a limb. There is this incredibly difficult and deeply rooted mental block on consenting to limb removal as a treatment option. We were at this place; sitting in the front office, debating whether to consent to cutting off the leg of her otherwise perfectly healthy and happy pup.
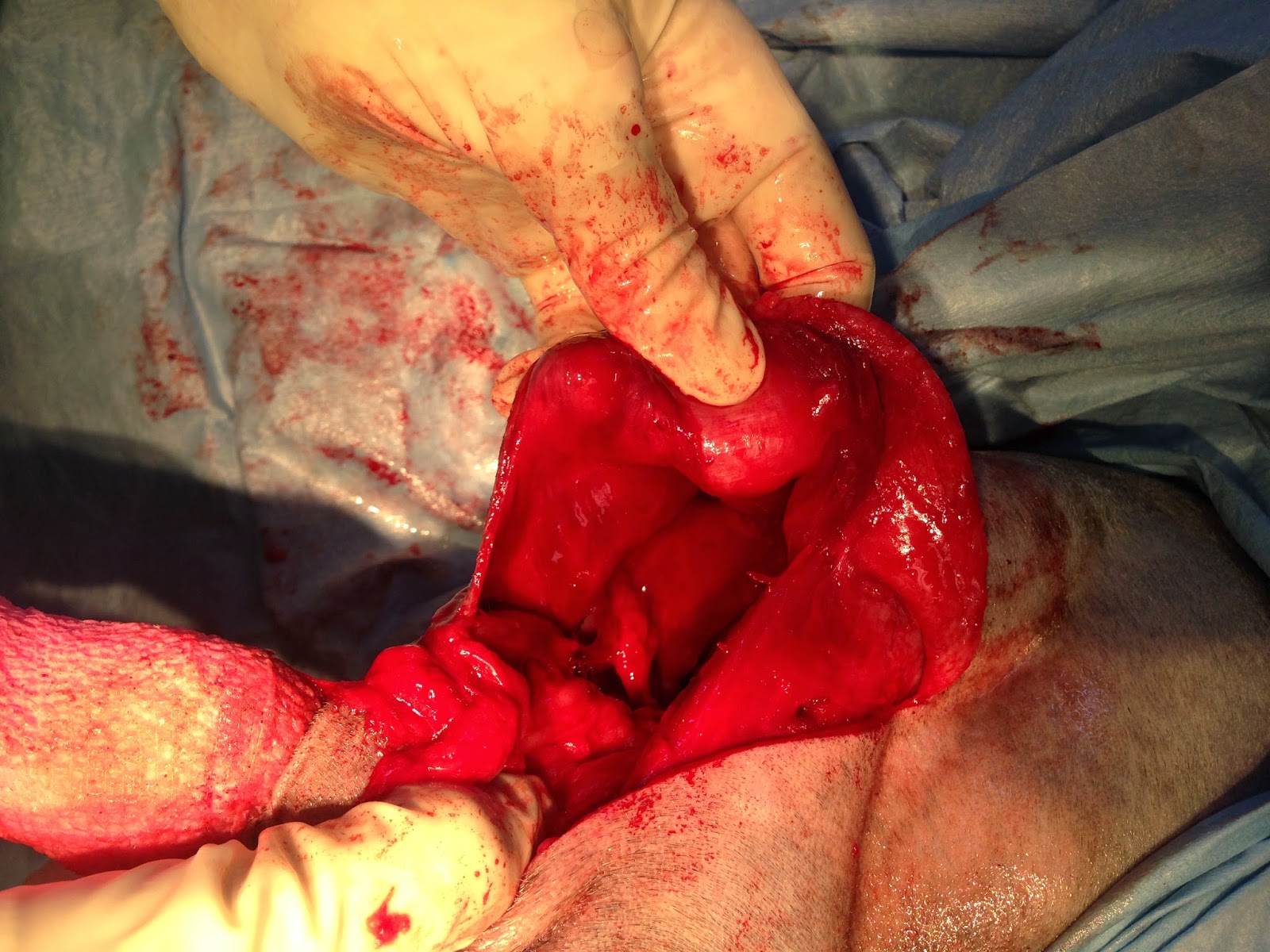
Brunswick is a timid 7 year old, 50 pound, mixed breed dog. She is a tawny brown with big erect triangular ears, a wide faced and her soft white body is liver spotted from neck to tail. She has a history of a mass removal from this leg that yielded a diagnosis of "lipoma" many years ago. That mass has returned, slowly growing within the armpit of her front leg. It is now pushing the limb out and away from her torso. It has gotten so large that it has exceeded her skins ability to further contain it. The underside of the arm was red, raw and ulcerating. The mass that has been slowly growing for years now is outgrowing her. The cold cruel eventuality of Brunswick's leg was lose the leg or lose her as she would soon have an open wound that would never heal but instead continue to erode her leg, cause her increasing pain, and chew its way up her neck and across her sternum.

Brunswick walks front legged short stepped, cowboy style. It manifests as a limp. The mass is hidden from obvious view by her bushy hair. The dappled coat hides the magnitude of the mass until you pet her. The diameter of the upper part of her left front leg is easily twice that of her slender athletic right leg. Her demeanor is always stand-offish for a few moments, but, if you are patient, quiet, and gentle in allowing those few moments to pass she will warm up to you to flounder flop on her "good" side for a full belly reveal. It is her not so subtle invitation to focus your affectionate rubs on the tender fleshy part of her belly. She is easy to fall in love with. Her handicap simply reinforces her charm. Her mom adores her. She will tell you that "Brunswick is her first child."
And, now,,, here we are. Sobbing. Crippled with fear and doubt, and stuck about what to do with it all.
Many conversations get to this point. That critical pivot point where biology, disease and prognosis has met the timetable of limited options. That juncture in a pets life where you have to choose? Are you a proactive parent seeking to gain as much time with your pet as medicine is able to provide? Or, do belong to the crowd that does not believe in surgical procedures for pets? Do you choose to invest multiple thousands of dollars, hours, and caregiving requirements to gain the precious commodity of more time with your companion. Do you value your pet as a member of your family? Are they one of your kids? Can anyone possibly speculate all of the twists and turns that lie ahead if you do, or don't, take action?

Most pre-op surgical discussions go like this.
In Brunswick's case we had already done multiple examinations. Two with me, one with the surgeon. At each time we (the "professionals") agreed the best resolution to this tumor was to remove the leg. There were about a dozen emails back and forth to discuss every possible question and concern. And,, yet,, here we were, crying at drop off.
I sat with her and said; "I know how hard this is. Please do what you think is right. Not what anyone else tells you to do." I firmly believe that this needs to be said to every parent. The road ahead is too full of twists, turns, and potentially even life-threatening landmines. I should add the cost of care, but, for me it is not a part of the equation I will let decide options. If we believe a treatment option is needed we will find a way to make it accessible. (Note: we use multiple payment plan options to help people not let the financial burden be the deciding factor).

I try to ask myself who will benefit from these decisions? Who am I looking after? These are huge weighty decisions with dire consequences. I try to be unbiased, neutral, indifferent. I try to present facts, argue all sides. I soo often feel that I fail miserably at this. I am not ever able to remain indifferent. I am not on anyone's team outside of my patients and their family. It is the dark force that grips my soul surrenders my conscious heart at midnight.
 |
| Brunswick post op |
Here's where the muck meets the sole. Brunswick needs this operation. She will die within a year from the mass if she doesn't have it. How do I advocate for that? A: I just have to be honest. Then I have to accept the consequences. But, I know Brunswick is loved and I know her mom is making this decision based on that. Seems silly to some, maybe? But that is always enough for me. I am not the vet for indifferent people who don't value pets. That I cannot do. That would kill me.
 |
| My pups; Frippie and Storm |
These are the elephants I carry on my back all day every day. They remain cumbersome, consuming and catabolic even after I get home at night.
I didn't sleep much after midnight. That mystical witching hour. My typical work day has me arriving home after 9 pm, a 12 hour day of work without breaks, meals or niceties logged in the record books. My shear exhaustion leads me to literally passing out on a pillow having foregone the obligatory teeth brushing, face washing, moisturizing and evening medical supplement regimen. They are all tossed out the window for the sake of sparing my legs the 80 paces they would require. There are loads of nights like this. Wrung out dry. I enter home as this zombie-eyed shell. I sleep for 3 hours and the death cipher lets go her grip for the anxiety ridden stressed-out-Suzie to take claim. Its always this exchange of custody each night between the hours of midnight and 2 am. A shared custody battle as the sun sleeps.
 |
| My Frippie always brings me a gift |
The other emotional dilemma of my day was an 11 month old German Shepherd, (let's call her GS), who visited for a pre-spay exam with bloodwork. Her mom had brought her inside the clinic vestibule on a one foot leash to a tight prong collar. Even with moms double fisted grip she could not get GS to remain with four feet on the floor nor have any kind of focus. She had no control of her adolescent puppy, and, she knew it. She told me that she "doubted I would be able to get her blood." She passed my technician the one foot lead and watched us all as we struggled to lead her to the treatment area. All GS needed was a 5 minute physical exam and 30 seconds to pull a blood sample. These appointments are not charged for as they should only take 6 minutes to complete. That didn't happen.
GS was a happy, outgoing 75 pound determined to party firecracker. She was elated to be around people, and in absolute resolve in not sitting for longer than one split second for anything. She knew commands, and she knew how to decide to avoid them. She surged, jumped, boxed, and thrashed. She twisted arms, crashed heads, and started to lunge and bite to have her demands heard.
 |
| Our dinnertime excitement |
I always stop here...... The three of us; myself, my technician, and GS. We all looked at each other. What to do now? Take a breath? Try a different tactic? All of the above? We took breaks. We tried treats. We tried calm quietness. I tried a large muzzle, just to see if that would settle her. Fifteen minutes into the endeavor and one thing was clear; Nothing worked. We were at the place where one of three things was going to happen;
1. I lose my patience and I hog tie, muzzle and we pig-pile on her to attempt to bruticaine (brute-force-paralysis vet lingo), and see if she is so shocked by this she gives in. I just turn into a cold hearted drill sergeant. Bark orders. Intimidate. Force her to be what I want her to be. Force her to hold this command until I feel she has learned who is in charge. Quickly restrain GS and get it done. Get the blood. Skip the exam. Smile and return her to mom. After all what she doesn't know isn't my problem. She can't claim naivete when she already admitted unruliness. Make friends with the owners, even if it is at the patients expense. A lot of vets have learned this trick. Two faced. Sweet to people, not so much to patients. A bite will likely follow at some point. What the real consequence of this is; To hell with the next guy who has to deal with her. Might work for some dogs, never works for shepherds. Shepherds are too intelligent, they cement resentment like dolphins. If I do this to her she will never again come happily into our doors.. She will start every future interaction with fear and aggression. A bite will follow at some point soon.
2. I give up knowing the short game loss is worth the long term gain and we have a family meeting to try to find a way to make her appointments more enjoyable and productive. Her mom had already expected that today wouldn't go well. We come up with a plan for next time. This should include training at home with the family to allow others to handle her. Working with a trainer to help her focus on commands and execution of them with focus and safety. And medications to help bridge the gap as we work on training.
3. I just get bitten. No chance to compromise, or convince her that we are not trying to hurt her. She just explodes and bites as fast as she can. She is done with us and she will remind us she is in charge.
What happens when a "bite" happens? Paperwork, fear, and almost always the pet parents compounds the tragedy by isolating their dogs in an attempt to avoid future potential bite provocations. Muzzles, prong collars, yelling, over protecting orders and mounting anxiety across all fronts. It's a snowball. Attempt to avoid situations leads to a lowering of estimation of the pets perceived threats. They used to like everyone. They were puppies meeting a world of new sights, sounds and smells. Now they are guardians that bark at the door knocking, or, strangers. You can't take them out in public anymore because now they bark at everyone. Everyone is a perceived threat. They are 100 pounds and you cannot restrain that amount of determined muscle. They become isolated. We reinforce the idea that everyone is a stranger. I used to see them every two to three weeks. We had fun visits. Now I am the stranger. I ask for unreasonable acts of discipline and focus. They don't know me and they certainly can't see a reason to obey me. Hence the bruticaine and indifference.
 |
| Buster |
Here's my advice; it is the advice that every seasoned pet care professional will give you. Train your dog to accept a muzzle. It is NOT a reflection of a persons failure. Nor the pets. It is a tool to provide assistance as we transition out of anxiety based fear laden actions and reactions. Every pet parent should openly and provide permission for a muzzle to be used if deemed necessary. Man-handling, bruticaine, that is not permissible.. ever (unless a pet is endangering another's life). How do we insure this? Trust. If you don't trust your pet care professionals ask to be present for all possible procedures. Ask, demand, insist that pre-anxiety medications be given. Set ground rules for care. Resistance is a flag for scrutiny. Leaving a practice because a person intervenes on your pets behalf is only going to hurt your pet.
About 30 minutes after I aborted pushing GS any further I sent her home with a training plan and sedatives to try at the next vet visit. I chose to not push her, not exacerbate a bite, and not make it impossible for the next time. Here's what I got for that, a call from the husband saying "they had a bad experience with us and they are going elsewhere." I doubt I will ever see GS again. There is pride before a fall. There are Shepherds relinquished everyday because no one intervened on their behalf at this critical development time. And, worst of fall there are vets who get court orders to put animals down after a "bite" history deems them a danger to the public. Will the next vet push her so hard she bites? Or becomes passive aggressive? Or fears people so much she reacts with defensive aggression to everyone outside of her family? In my opinion she needs help. Will she get it? It's one of the reasons I awaken at midnight with elephants.
 |
| Tex. His first puppy visit. My goal is to have every patients visit look like this. |
The truth is that people pine as much as I do, if not more, on what to do for their companions. What is the right/best/safest/compassionate course of action to take? What will consequences for that looks like? Will I hate/berate/beat up/chastise myself for the action, or lack there of, I take? I have been in these shoes. At every moment of my professional life I remind myself that I am still that devoted pet parent who is in turmoil about what to do? Do I trust my own judgement? Do I have enough pertinent information to base my judgements upon? Is there trust here. Maybe GS's parents lack that? They just don't trust my call? The reality is that she is being set up to fail, not flourish, and her "bite" won't be on my account of failing her.
 |
| Brunswick. One week post-op forelimb amputation |
What these two cases have in common is that I did my best to make decisions, present options that were in the best interest of my patients. period. I can fall asleep knowing that. The rest, the worry, the grief, the elephant on my shoulders that I failed them, their parents, or the relationships we have is the midnight hour that clutches my throat and drags me into the abyss of self-doubt of avenues from that first decision to "do no harm."
 |
| Magpie helps me motivate for another morning. |